|
These are some questions both for technicians and physicians concerning neurography.
If you get 50% correct in your answers, you have a good knowledge.
Naturally the answers can always be discussed, but the most reasonable alternative is enough.
|
1. Sometimes you see stable and complex late components after each CMAP at consecutive stimulations. What to do?
Show/Hide Answer
2. Sometimes you see irregular and changing (variable) late components after each CMAP at consecutive stimulations. What to do?
Show/Hide Answer
3. Sometimes irregular signals are seen both before and after the CMAP. What is this, and what to do?
Show/Hide Answer
4. If CMAP from thenar muscles at distal stimulation of the median nerve is lower than(or even identical as) at prox stimulation, what to do?
Show/Hide Answer
5. If CMAP from thenar muscles at distal stimulation of the median nerve is higher than that at prox stimulation, what to do?
Show/Hide Answer
6. If CMAP of the EDB is lower at distal than at prox stim, what to do?
Show/Hide Answer
7. If CMAP amplitude has an unexpectedly low amplitude (no nerve damage, no pnp), what to do?
Show/Hide Answer
8. The CMAP from APB may have an initial positive deflection at proximal but not at distal stimulation.
- Why?
- Where do you set the latency cursor?
Show/Hide Answer
9. If sural response in your patient without PNP is questionably present. What to do?
Show/Hide Answer
10. We have different “disturbances” in recording the CMAP. Give one-word answer to where they are generated and one-word answer to how to reduce them.
- Noise
- Interference
- Randomly varying baseline
- Volume conduction
- Standing wave (Far field potential)
Show/Hide Answer
11. If the MCV is slower (diff > 10 m/sec) in ulnar nerve across the elbow than distally, what to do?
Show/Hide Answer
12. Median nerve. If the CV is 85 m/sec, what do you expect?
Show/Hide Answer
13. If the sensory median amplitudes are high (1.8 SD) and the latency prolonged, what to do?
Show/Hide Answer
14. If the foot goes downwards (plantar flexion) on stimulation of the fibular nerve distal to the fibula head, how can you differentiate between the two possible explanations?
Show/Hide Answer
15. In a slight CTS the palm stimulation (wrist recording) may have normal latency while dig III stimulation is abnormal. Why?
Show/Hide Answer
16. Can an A-wave appear after the F-responses. If so, where is it generated?
Show/Hide Answer
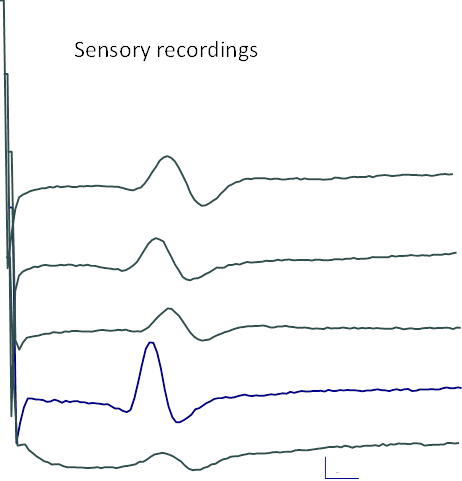
17. Different signals will be shown here. Within each example the recordings come from different patients. Where is the recording obtained?
Show/Hide Answer
18. Both APB and Pron Quadr are innervated by the Median nerve. If you stimulate the Median nerve at the wrist, can you obtain F-responses then also in Pron Quadr?
Show/Hide Answer
19. 5 sensory nerves, ortodromic or antidromic. Which nerves are studied?
Show/Hide Answer
20. Because of amplifier and electrode characteristics, low amplitude signals such as SNAPs will be disturbed by noise.
This will influence accurate measurements. How can the signals be improved by noise reduction? Give 3 answers.
Show/Hide Answer
21. Why is it essential to have standard interelectrode distance for sensory recordings?
Show/Hide Answer
22. Standard motor studies; recording from “AH”, what is that?
Show/Hide Answer
23. For motor studies, how does the size of the surface electrode influence the recorded signal?
Show/Hide Answer
24. Facial nerve is considered as pure motor nerve.
Why it is the then painful to stimulate the facial with surface electrical stimulation of the facial nerve?
Show/Hide Answer
25. In a patient with hand trauma mainly leading to loss of function of thumb movement (abduction impaired) and therefore evaluation of median nerve is requested.
You get a good CMAP from APB and good sensory response from dig III. Possible explanation.
Show/Hide Answer
26. Fasciculation potentials are seen during rest. Can they generate F-responses?
Show/Hide Answer
27. Stimulated fasciculation potentials. Can they generate F-responses?
Show/Hide Answer
28. Voluntary a-waves, during rest. Can they generate F-responses?
29. Stimulated a-waves. Can they generate F-responses?
Show/Hide Answer
30. F-waves. CMAP in a postpolio patient is low. What about F-waves; persistence, amplitudes?
31. F-waves. CMAP in a patient with myopathy is low. What about F-waves; persistence, amplitudes?
Show/Hide Answer 32&33
32. Filters in sensory recording, which is optimal low pass filter?
Show/Hide Answer
33. Why is R2 in the blink reflex so complex in shape?
Show/Hide Answer
34. The fingers are cooled in water and the orthodromic sensory signal from dig III to the wrist is recorded. Which is the effect of the signals regarding amplitude, amplitude and latency?
Show/Hide Answer
35. Do the F-responses have a low amplitude e.g. in GBS with conduction block?
Show/Hide Answer
36. How do you interpret a finding of low sensory amplitude at dig III after antidromic testing both at wrist and at palm stimulation? Ulnar sensory from palm is normal.
Show/Hide Answer
37. Difference between testing different segments for CTS.
In moderate CTS, is there amplitude difference between antidromically tested wrist–palm and antidromically tested palm-dig III?
Show/Hide Answer
38. If SFEMG is normal but RNS is 8%. What to do? (Notice, that a normal SFEMG result in principle does not need any succeeding RNS)
Show/Hide Answer
39. Which is the optimal time for maximal voluntary activation in RNS tests in MG and LEMS? Show/Hide Answer
40. Why is it logic to start an MG diagnostic EDX with SFEMG before RNS (if SFEMG is available and already booked to be performed)? Show/Hide Answer
41. Sternocleidomastoideus muscle is moving the head (rotation). So, is the head moving when you perform correctly RNS from trapezius muscle?
42. Is it normal to have some degree of “biting” when you perform RNS of the nasalis muscle? If not, what to do?
Show/Hide Answer 48&49
43. In 3HZ RNS the second response is sometimes higher than the first (see one of the RNS pictures). What is this called? Which is the mechanism?
Show/Hide Answer